
When he was sixteen, a young man we’ll call Mitch couldn’t sleep.
He worried about nuclear war. He was convinced it would happen soon and dreaded the day. He spoke of it all the time to friends and family, who shrugged him off as silly. And then the thoughts began to obsess him. His grades dropped, and he couldn’t concentrate on school work anymore. As the years passed, Mitch got more nervous and anxious. He worried about crossing narrow bridges and intersections, and cringed at traffic lights. He stopped driving altogether. Eventually he stopped working. His psychiatrist helped him file for mental disability. He lived on social security for three and a half years.
Mitch is one of a large group of people with obsessive-compulsive disorder, or OCD. People with OCD have obsessive thoughts, which are often accompanied by repetitive behavior. In the United States alone, about one in fifty adults has OCD, according to the Obsessive Compulsive Foundation. Traditional treatments rely on antidepressants such as Paxil and Prozac, which are known to have side effects. Jonathan Abramowitz, a clinical psychologist at UNC’s Anxiety and Stress Disorders Clinic, uses a different approach. Abramowitz teaches OCD patients to overcome their fears.
“Wondering if you left the iron on at home might be a normal thought most of us have,” Abramowitz says. “But people with OCD worry if the speed bump they just ran over was a human body.” Some patients can’t even go to work because their compulsive behavior takes too much time or because they’re worried they’ll catch germs. Others have recurrent senseless thoughts, which they constantly struggle to suppress.
Because of embarrassment and fear of unwanted thoughts, OCD patients tend to have constant low self-esteem. “It doesn’t go away on its own,” Abramowitz says. People who don’t seek treatment are constantly fighting a losing battle.
For those who do seek treatment, Abramowitz uses cognitive behavioral therapy, or CBT, which clinical trials have shown to be more effective than talk therapy or medication. “In CBT, we teach people lifelong skills to control the anxiety associated with obsessive thoughts,” Abramowitz says. He puts OCD patients in simulated situations that resemble real life as closely as possible, and trains them to manage their anxiety when it comes time to face their thoughts. He also teaches them to repeat certain statements and actions to overcome their fears. “If someone’s afraid of door handles because they may contain germs, we help them to touch a bunch of door handles so they can see that realistically it’s safe,” Abramowitz says. And he’s found that the patients in his program who don’t take medication do just as well as those who do.
But CBT doesn’t work as well for patients who have no insight into their condition. “For those who don’t even realize that their actions and thoughts are irrational, CBT might not be the best answer,” Abramowitz says. “Probably because they’re too fearful to follow through the course of the treatment.”
Many partners of OCD patients play along with the patients’ fears and obsessive behavior in order to make life easier, Abramowitz says. Couples therapy aims at educating partners and helping patients deal with OCD as a team. “That’s not only a bonding experience for the patient but also an effective way to communicate in an anxious situation,” Abramowitz says.
We still don’t know what causes OCD. It may arise from a combination of factors, and no one gene or protein has been identified as the cause in humans. “Anxiety is a helpful thing; it protects us from harm,” Abramowitz says. “But people who tend to be more anxious than others are more apt to develop OCD.”
An effective test to identify patients susceptible to the disorder, though, is unlikely. “Psychological problems demand a psychological answer,” he says. “We can’t simply reduce it to biology.”
But neuroscientists are looking for biological explanations, and Guoping Feng at Duke decided to look for them in mice. Feng teamed up with Richard Weinberg at UNC’s Neuroscience Center and other researchers to uncover an instance of OCD-like behavior in mice. The scientists suspected the answer lay in nerve impulse transmission, and wondered if rejiggering the junctions of nerve impulse relays could lead to OCD-like symptoms.
Feng had long been fascinated by synapses, the structures that relay nerve impulses across nerve cells. The signal-receiving end of the synapse, called the postsynaptic complex, houses receptors that transmit impulses. The complex is less than a micrometer across and has hundreds of proteins enmeshed by molecular scaffolds and buttresses, most of whose functions are still unknown. Feng unhinged the complex by removing a protein called SAPAP3. He expected these mutant mice to be different but he had no clue how they would behave.
By the time Feng’s mice were six months old, lesions and patches of hairless skin appeared under their eyes and snouts, then spread. Feng’s team videotaped the mice and observed a remarkable thing: “The mutant mice would spend more than a third of their time scratching themselves sore and self-inflicting these lesions while the normal mice slept on,” Feng says. “The mutants would compulsively groom themselves.”
The OCD mice were also more anxious. They skulked in dark areas and along the walls of the experimental chambers while the other mice scuttled around open spaces. Seeking shelter in the chambers is a sign of anxiety in the mice, Feng says.
“When we gave these mice Prozac, they recovered and the lesions disappeared,” Feng says. But the researchers needed to know what losing SAPAP3 did to the mice’s brains, and Weinberg had the answer.
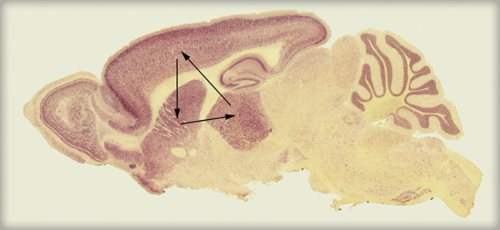
“When you remove one protein from a region in the brain,” Weinberg says, “you may not always see an effect, because other proteins do the same job, or because the protein you removed didn’t do much. With SAPAP3, it was different: it was the only one of its kind present in a region of the brain called the striatum.” The striatum is involved in addiction and in situations that require resisting temptation or overcoming a strong habit. Not only did the mutant mice have altered synapses that were less able to transmit signals, but Weinberg’s team found subtle defects in the structure of the postsynaptic complexes in the striatum. “My guess is that other proteins may be missing in the synapses of these mutant mice since the scaffolding protein was removed, but that hasn’t been identified yet,” he says.

Feng wanted clinching evidence that SAPAP3 was indeed involved in these behaviors. So his team returned working versions of the lost SAPAP3 gene into the mutant mice by injecting a virus bearing it into the mice’s brains to see if their lost function could be restored. Six months later, five of the eight mice recovered. They had no lesions, were less anxious, and their synapses transmitted impulses normally.
Feng’s team is now trying to identify mutations in human SAPAP3 in families with a history of OCD. Christopher Pettinger, director of the Yale OCD Research Clinic, says, “This is the best characterized and most convincing mouse model of OCD that has been described to date. It would be exciting if we learned that SAPAP3 is one of the mutated genes in OCD patients, but we’re not there yet.”
Scientists are also nowhere close to doing the kind of therapeutic gene-jockeying in humans that they did with the mice, Weinberg says. “Right now that stuff is pie in the sky. Do we really want to inject a virus bearing SAPAP3 into a person’s brain? How long do we have to study the person before we know that we don’t hurt the neurons? Maybe some day in the far future, but I’d be surprised if it happens in the next twenty years,” he says.
But drug companies could identify chemicals that interact with SAPAP3 and correct its function by testing them in mice. Feng has already started collaborations with drug manufacturers who will use the mice to screen libraries of such chemical compounds.
“That would be a more science-based therapy with an understanding of what goes wrong in OCD,” Weinberg says. Current therapies are based on trial and error.
Abramowitz, though, is not convinced. Most of the repetitive behaviors seen in OCD patients happen in response to obsessive thoughts. But not all OCD patients have rituals. A driver who clutches a steering wheel harder because he fears he may turn the car into oncoming traffic could have OCD, Abramowitz says. But the important thing is that the action happens in response to an obsessive thought. “We don’t know if mice have obsessive thoughts,” he says.
Prashant Nair is a master’s student in medical journalism at Carolina.
Jonathan Abramowitz is an associate professor in the Department of Clinical Psychology. Richard Weinberg is a professor in the Department of Cell and Developmental Biology in the School of Medicine. Guoping Feng is an assistant professor of neurobiology at Duke University.